The NEW ENGLAND JOURNAL of MEDICINE
Catharine I. Paules, M.D., Hilary D. Marston, M.D., M.P.H., Marshall E. Bloom, M.D., and Anthony S. Fauci, M.D.
 very spring, public health officials prepare for an upsurge in vectorborne diseases. As mosquito-borne illnesses have notoriously surged in the Americas, the U.S. incidence of tickborne infections has risen insidiously, triggering heightened attention from clinicians and researchers.
very spring, public health officials prepare for an upsurge in vectorborne diseases. As mosquito-borne illnesses have notoriously surged in the Americas, the U.S. incidence of tickborne infections has risen insidiously, triggering heightened attention from clinicians and researchers.
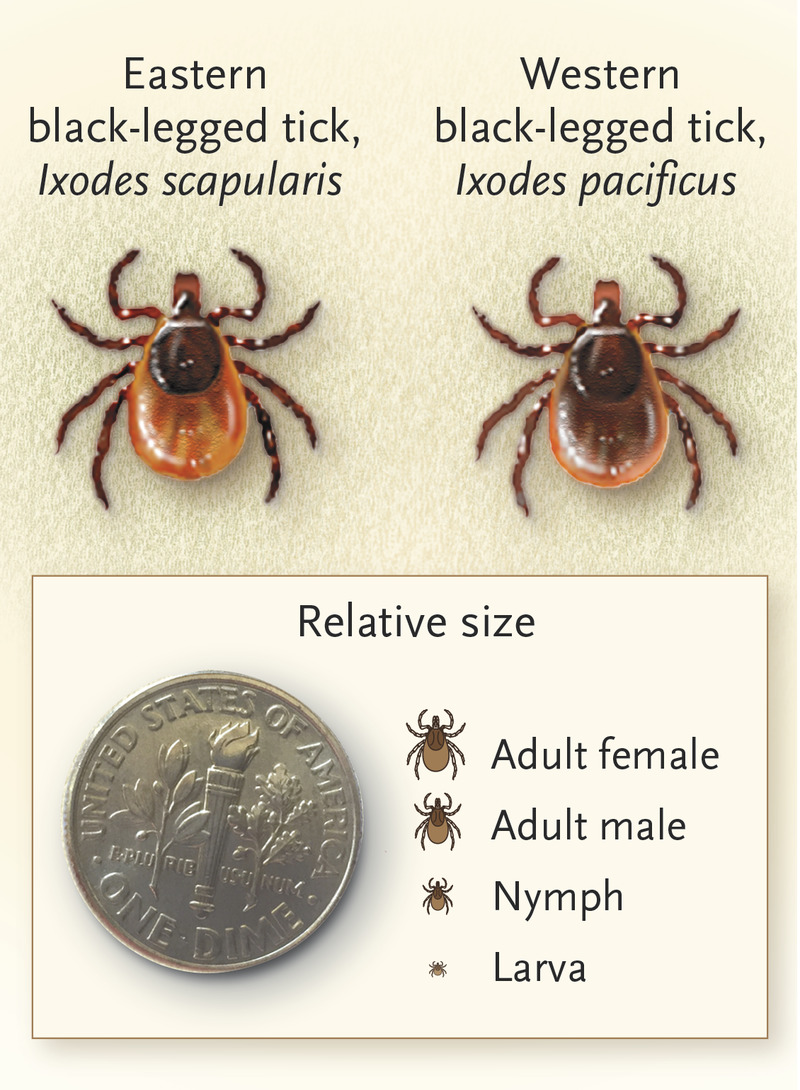 According to the Centers for Disease Control and Prevention (CDC), the number of reported cases of tickborne disease has more than doubled over the past 13 years.1 Bacteria cause most tickborne diseases in the United States, and Lyme disease accounts for 82% of reported cases, although other bacteria (including Ehrlichia chaffeensis, Anaplasma phagocytophilum, and Rickettsia rickettsii) and parasites (such as Babesia microti) also cause substantial morbidity and mortality. In 1982, Willy Burgdorfer, a microbiologist at the Rocky Mountain Laboratories of the National Institute of Allergy and Infectious Diseases, identified the causative organism of Lyme disease, a spirochete eponymously named Borrelia burgdorferi. B. burgdorferi (which causes disease in North America and Europe) and B. afzelii and B. garinii (found in Europe and Asia) are the most common agents of Lyme disease. The recently identified B. mayonii has been described as a cause of Lyme disease in the upper midwestern United States. Spirochetes that cause Lyme disease are carried by hard-bodied ticks (see graphic), notably Ixodes scapularis in the northeastern United States, I. pacificus in western states, I. ricinus in Europe, and I. persulcatus in eastern Europe and Asia. B. miyamotoi, a borrelia spirochete found in Europe, North America, and Asia, more closely related to the agents of tickborne relapsing fever, is also transmitted by I. scapularis and should be considered in the differential diagnosis of febrile illness occurring after a tick bite.
According to the Centers for Disease Control and Prevention (CDC), the number of reported cases of tickborne disease has more than doubled over the past 13 years.1 Bacteria cause most tickborne diseases in the United States, and Lyme disease accounts for 82% of reported cases, although other bacteria (including Ehrlichia chaffeensis, Anaplasma phagocytophilum, and Rickettsia rickettsii) and parasites (such as Babesia microti) also cause substantial morbidity and mortality. In 1982, Willy Burgdorfer, a microbiologist at the Rocky Mountain Laboratories of the National Institute of Allergy and Infectious Diseases, identified the causative organism of Lyme disease, a spirochete eponymously named Borrelia burgdorferi. B. burgdorferi (which causes disease in North America and Europe) and B. afzelii and B. garinii (found in Europe and Asia) are the most common agents of Lyme disease. The recently identified B. mayonii has been described as a cause of Lyme disease in the upper midwestern United States. Spirochetes that cause Lyme disease are carried by hard-bodied ticks (see graphic), notably Ixodes scapularis in the northeastern United States, I. pacificus in western states, I. ricinus in Europe, and I. persulcatus in eastern Europe and Asia. B. miyamotoi, a borrelia spirochete found in Europe, North America, and Asia, more closely related to the agents of tickborne relapsing fever, is also transmitted by I. scapularis and should be considered in the differential diagnosis of febrile illness occurring after a tick bite.
Patterns of spirochete enzootic transmission are geographically influenced and involve both small-mammal reservoir hosts, such as white-footed mice, and larger animals, such as white-tailed deer, which are critical for adult tick feeding. The rising incidence and expanding distribution of Lyme disease in the United States are probably multifactorial, but increased density and range of the tick vectors play a key role. The geographic range of I. scapularis is apparently increasing: by 2015, it had been detected in nearly 50% more U.S counties than in 1996.
Lyme disease’s clinical manifestations range from relatively mild, nonspecific findings and classic erythema migrans rash in early disease to more severe manifestations, including neurologic disease and carditis (often with heart block) in early disseminated disease, and arthritis, which may occur many months after infection (late disease). Although most cases are successfully treated with antibiotics, 10 to 20% of patients report lingering symptoms after receiving appropriate therapy.2 Despite more than four decades of research, gaps remain in our understanding of Lyme disease pathogenesis, particularly its role in these less well-defined, post-treatment symptoms.
Meanwhile, tickborne viral infections are also on the rise and could cause serious illness and death.1 One example is Powassan virus (POWV), the only known North American tickborne encephalitis-causing flavivirus.3 POWV was recognized as a human pathogen in 1958 after being isolated from the brain of a child who died of encephalitis in Powassan, Ontario. People infected with POWV often have a febrile illness that can be followed by progressive and severe neurologic manifestations, resulting in death in 10 to 15% of cases and long-term sequelae in 50 to 70% of survivors.3 An antigenically similar virus, POWV lineage II, or deer tick virus, was discovered in New England in 1997. Both POWV subtypes are linked to human disease, but their distinct enzootic cycles may affect their likelihood of causing such disease. Lineage II seems to be maintained in an enzootic cycle between I. scapularis and white-footed mice — which may portend increased human transmission, because I. scapularis is the primary vector of other serious pathogens, including B. burgdorferi. Whereas only 20 U.S. cases of POWV infection were reported before 2006,3 99 were reported between 2006 and 2016. Other tickborne encephalitis flaviviruses cause thousands of cases of neuroinvasive illness in Europe and Asia each year, despite the availability of effective vaccines in those regions. The increase in POWV cases coupled with the apparent expansion of the I. scapularis range highlight the need for increased attention to this emerging virus.
The public health burden of tickborne pathogens is considerably underestimated. For example, the CDC reports approximately 30,000 cases of Lyme disease per year but estimates that the true incidence is 10 times that number.1 Multiple factors contribute to this discrepancy, including limitations in surveillance and reporting systems and constraints imposed by available diagnostics, which rely heavily on serologic assays.4 Diagnostic utility is affected by variability among laboratories, timing of specimen collection, suboptimal sensitivity during early infection, imperfect use of diagnostics (particularly in persons with low probability of disease), inability of a single test to identify coinfections in patients with acute infection, and the cumbersome nature of some assays. Current diagnostics also have difficulty distinguishing acute from past infection — a serious challenge in diseases characterized by nonspecific clinical findings. Moreover, tests may remain positive even after resolution of infection, leading to diagnostic uncertainty during subsequent unrelated illnesses. For less common tickborne pathogens such as POWV, serologic testing can be performed only in specialized laboratories, and currently available tests fail to identify novel tickborne organisms.
Such limitations have led researchers to explore new technologies. For example, one of the multiplex serologic platforms that have been developed can detect antibodies to more than 170,000 distinct epitopes, allowing researchers to distinguish eight tickborne pathogens.4 In addition to its utility in screening simultaneously for multiple pathogens, this assay offers enhanced pathogen detection, particularly in specimens collected during early disease. Further studies are needed to determine such assays’ applicability in clinical practice.
Nonserologic platform technologies may also improve diagnostic capabilities, particularly in identifying emerging pathogens. Two previously unknown tickborne RNA viruses, Heartland virus and Bourbon virus, were discovered by researchers using next-generation sequencing to help link organisms with sets of unexplained clinical symptoms. The development and widespread implementation of next-generation diagnostics will be critical to understanding the driving factors behind epidemiologic trends and the full clinical scope of tickborne disease. In addition, sensitive, specific and, where possible, point-of-care assays will facilitate appropriate clinical care for infected persons, guide long-term preventive efforts, and aid in testing of new therapeutics and vaccines.
In the United States, prevention and management of tickborne diseases include measures to reduce tick exposure, such as avoiding or controlling the vector itself, plus prompt, evidence-based treatment of infections. Although effective therapies are available for common tickborne bacteria and parasites, there are none for tickborne viruses such as POWV.
The biggest gap, however, is in vaccines: there are no licensed vaccines for humans targeting any U.S. tickborne pathogen. One vaccine that was previously marketed to prevent Lyme disease, LYMErix, generated an immune response against the OspA lipoprotein of B. burgdorferi, and antibodies consumed by the tick during a blood meal targeted the spirochete in the vector.5 Nonetheless, the manufacturer withdrew LYMErix from the market for a combination of reasons, including falling sales, liability concerns, and reports suggesting it might be linked to autoimmune arthritis, although studies supported the vaccine’s safety. Similar concerns will probably affect development of other Lyme disease vaccines.5
Historically, infectious-disease vaccines have targeted specific pathogens, but another strategy would be to target the vector.5 This approach could reduce transmission of multiple pathogens simultaneously by exploiting a common variable, such as vector salivary components. Phase 1 clinical trials are under way to evaluate mosquito salivary-protein–based vaccines in healthy volunteers living in areas where most mosquito-borne diseases are not endemic. Since tick saliva also contains proteins conserved among various tick species, this approach is being explored for multiple tickborne diseases.5
The burden of tickborne diseases seems likely to continue to grow substantially. Prevention and management are hampered by suboptimal diagnostics, lack of treatment options for emerging viruses, and a paucity of vaccines. If public health and biomedical research professionals accelerate their efforts to address this threat, we may be able to fill these gaps. Meanwhile, clinicians should advise patients to use insect repellent and wear long pants when walking in the woods or tending their gardens — and check themselves for ticks when they are done.